What is Hip Dysplasia?
The hip is a true ball and socket joint. The femoral head (ball) and the acetabulum (socket) make up the hip joint. In some people, the socket does not form as fully as it should, leaving some of the ball uncovered by the socket. The name of his condition is hip dysplasia. In childhood it is called developmental dysplasia of the hip (DDH).Whereas, during adolescence and adulthood, it is called acetabular dysplasia.
In severe cases, the femoral head is dislocated from the socket at birth. If dysplasia is caught early enough after birth, it is treated with a specialized harness. It is more common in women than men. Hip dysplasia can cause hip pain in adolescence through adulthood.
Watch this 2-minute video on hip dysplasia with our orthopedic specialist, Dr. Carl Freeman
Part 2: Inside the Procedure: What to Expect from PAO Surgery
Part 3: Life After PAO Surgery: Building Back Mobility

Epidemiology of Hip Dysplasia:
- DDH occurs in approximately 1 in 1000 births.
- Due to the increased force placed through a smaller surface area of the acetabulum, hip dysplasia has been found to increase the individual’s likelihood of developing hip osteoarthritis.
- Hip dysplasia is one of the most common causes for hip replacement.
Diagnosis of Hip Dysplasia
Specialized X-ray measurements and physical exam findings can diagnose hip dysplasia.
- Tonnis Angle– also known as the acetabular roof angle, is a measurement of femoral head bony coverage by the acetabulum.
- Normal: 0-7 degrees
- Increased: >10 degrees Suggestive of hip dysplasia, with decreased coverage of the acetabulum over the femoral head.
- Decreased: <0 degrees Suggestive of pincer impingement, with increased coverage of the acetabulum over the femoral head.
Signs and symptoms of Acetabular Dysplasia:
In childhood, hip dysplasia is often asymptomatic, or only associated with a limp. However, as the individual becomes an adolescent and an adult, the increased forces across the hip causes structural breakdown in a patient with hip dysplasia, and the following symptoms become common:
- Pain at the front of the hip or the groin
- Pain with prolonged standing, walking, or running
- Persistent muscle soreness at front and outside of hip
Surgical Treatment Strategies:

- Hip Arthroscopy– This is a minimally invasive procedure where the surgeon can use an arthroscope to repair a labral tear, but this does not correct the underlying deformity.
- Osteotomy– The most common is Periacetabular Osteotomy (PAO)- This is an open hip surgery that corrects the underlying deformity of hip dysplasia. During this procedure, the surgeon makes precise bone cuts around the hip in order to improve coverage of the acetabulum over the femur. This is typically performed in patients under 40 years old with minimal cartilage damage, and is only performed by surgeons who specialize in Hip Preservation Surgery.
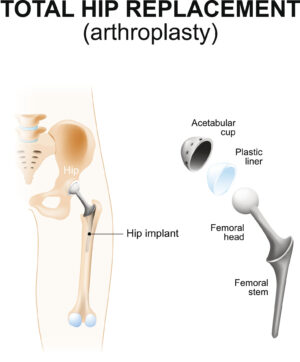
- Total hip replacement (THR)– Often performed in patients older than 40 years old or patients with significant structural damage and arthritis caused by hip dysplasia.
Conservative Treatment Strategies:
- Activity Modifications– Avoid tasks that require high impact into hip joint including sport related activities (i.e., running, jumping, hopping)
- Anti-Inflammatory Medications (NSAIDS)– Decreases inflammation to alleviate pain within the hip joint.
- Physical Therapy– Work with your physical therapist to address impairments including pain, muscle weakness, or decreased mobility at the hip joint.
- Injections– Your doctor may perform an injection, such as a cortisone injection, to decrease inflammation and pain within the joint. Typically, this will give temporary relief.
Physical Therapy for Patients with Hip Dysplasia:
- Lumbo-Pelvic Positioning: The suggestion is that pelvic and spinal adaptations may occur to improve stability of the ball and socket joint. Lumbo-pelvic positioning can also occur due to muscular imbalances of the hips and low back.
- Anterior Pelvic Tilt: pelvis is in a forward position. This causes the lumbar spine to extend which creates increased lumbar lordosis, also known as an increased curve at the low spine. Patients with dysplasia may utilize an anterior pelvic tilt to improve bony coverage onto the femoral head
- Posterior Pelvic Tilt: the pelvis is in a backward position. This causes the lumbar spine to flex and will decrease lumbar lordosis, this causes a “flat back” position.
Your physical therapist can implement a core stability program to strengthen or adjust the positioning of your spine to pelvis to optimize movement patterns.
Muscular involvement:
- Hip Abductors: Located at the side of your hips, these muscles play a key role in pelvic stability, especially during single leg tasks such as walking and running. With a shallow hip socket, these muscles must work harder and might experience earlier fatigue.
- Hip Flexors: Located at the front of the hip. These muscles must work harder to maintain stability at the front of a dysplastic hip joint. Due to increased demand for the hip flexors. Muscles may tighten which can cause clicking or snapping sensations at the front of the hip joint.
Related Articles:
Watch this Hip Exercise Series brought to you by The Jacksonville Orthopaedic Institute.
Book an Appointment with The Jacksonville Orthopaedic Institute Today!
JOI Physicians continue to offer online new patient appointments. This is another option to make it more convenient to make new patient appointments with less phone hold times. Follow the link below to select your JOI MD and schedule online.
You can still call 904-JOI-2000 to make new patient JOI Physician Appointments if that is your preference.
New To JOI: You now can make and cancel follow-up appointments for your JOI Physician through the JOI Portal.
To make appointments with JOI Rehab, please call 904-858-7045.