Understanding ACL Reconstruction
ACL reconstruction is a surgical method used to fix a torn anterior cruciate ligament (ACL) in the knee. This surgery is frequently done to bring back stability and normal functioning to the knee after an ACL injury. Here at joijax.com, we appreciate the significant role of ACL reconstruction in enhancing the overall health and wellness of our patients.
What You Need to Know About ACL Reconstruction
ACL reconstruction surgery involves repairing a torn anterior cruciate ligament (ACL) in the knee. The ACL is a key ligament that aids in stabilizing the knee. When it gets damaged or torn, often due to sports injuries or accidents, ACL reconstruction surgery may be suggested.
The primary aim of ACL reconstruction surgery is to regain stability and functionality in the knee. It’s typically done when non-surgical treatments like physical therapy and bracing don’t bring about sufficient relief, or when the patient leads an active lifestyle or is an athlete.
During the procedure, the damaged ligament is replaced with a graft, which can either be obtained from the patient’s body (autograft) or from a donor (allograft). The most common autografts include the patellar tendon and the hamstring tendon, while allografts are usually obtained from a cadaver.
The surgery is often done using minimally invasive techniques like arthroscopy, which involve small incisions and the use of a camera to guide the surgeon. The graft is inserted through tunnels drilled in the femur and tibia bones and is kept in place with screws or other fixation devices.
The method of ACL reconstruction surgery varies, and the choice of graft depends on several factors such as the patient’s age, activity level, and the surgeon’s preference. The surgeon will discuss the options and recommend the best approach for each patient.
ACL Tears
Anterior cruciate ligament (ACL) tears are one of the most common serious sports injuries. It is estimated that 200,000 ACL injuries occur in the United States each year. The ACL plays a vital role in maintaining knee stability. An ACL deficient knee can result in recurrent instability, meniscus tears and articular cartilage degeneration. There were many different types of procedures for ACL’s in the past. Beginning in the late 1980’s, arthroscopic ACL reconstruction was the most successful procedure. It uses the middle third of the patellar tendon as the new ligament. This procedure continues to be refined to the current procedure today.

Causes of ACL Injuries
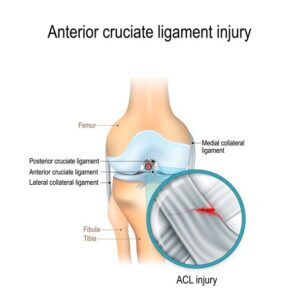
These injuries commonly occur during deceleration, cutting, or twisting maneuvers (Figure 1). Patients will often report sensing a pop within the knee and then subsequently swelling, or “water on the knee”, with a sensation of instability when they are walking. When associated with an injury to the medial collateral ligament, these injuries are much more painful. However, patients with isolated ACL injuries may improve over a week or two and the athlete does not recognize the seriousness of the injury until they try to return to sport and experience a buckling or instability sensation in their knee.
Diagnosis of ACL Tears
The first step to diagnose an ACL tear is a thorough physical examination of the knee. This often includes X-rays and an MRI. A tear of the ACL has become the most feared injury in sports. These surgical procedures have allowed most athletes to return to their respective sports, although usually not before 6 to 12 months of vigorous rehabilitation.
Not all patients with an ACL tear require surgical reconstruction. However, most younger and active patients will require this for the knee to achieve the stability to return to full activity. In addition, physiological age is probably more important than chronological age. The recreational activities and activity level will ultimately dictate whether surgery is necessary. Sometimes, the MRI will show associated injuries such as ligamentous injury, meniscal injuries or cartilage damage. This would require, at the least, arthroscopic treatment.
Some physicians will allow the swelling to decrease before operating on the knee. It is not uncommon for the physician to wait three to six weeks prior to ACL reconstruction. This delay will help prevent stiffness and may improve the rehabilitation process.
Getting Ready for ACL Reconstruction
If you’re advised to undergo ACL reconstruction surgery, it’s crucial to understand what to expect before the procedure, the necessary medical tests, and how to prepare for a successful surgery.
Your doctor will provide detailed information about the surgery, its potential benefits, and risks. They will also explain the recovery process. Be sure to ask any questions you have during this consultation to ensure you understand fully.
Medical tests and evaluations are often done before ACL reconstruction surgery to assess your overall health and identify any potential risks. These may include blood tests, X-rays, MRI scans, and a physical examination. Your doctor will use these tests to determine if you’re suitable for surgery and to plan the most effective surgical approach.
Follow your doctor’s instructions closely to prepare for ACL reconstruction. They may advise you to stop taking certain medications or supplements that can increase the risk of bleeding. You may also need to refrain from eating or drinking for a specific period of time before the surgery. Be sure to inform your doctor about any allergies or medical conditions you have, and to arrange for transportation to and from the surgical facility.
Preparing for ACL reconstruction surgery involves not only physical preparation but also mental and emotional readiness. It can be helpful to educate yourself about the procedure, understand the expected recovery timeline, and gather support from friends and family. Creating a comfortable and accessible recovery space at home can also contribute to a smoother post-surgery experience.
Different Graft Options for ACL Reconstruction
Once the surgeon and the patient have decided that ACL reconstruction will be required, the first important decision the doctor and the patient make is on the type of graft for the ACL reconstruction. In the younger and more athletic patient population a central third patella tendon autograft is often the graft of choice.

Patella Tendon Autograft
This graft is chosen because of its strength, characteristics, rigid fixation, bone-to-bone healing and favorable clinical outcome. This does, however, make the largest scar of the graft choices. It is often is somewhat more painful than other types of reconstruction and may result in some anterior knee pain and pain while kneeling. The use of autograft tissue has been shown to have faster healing, greater graft strength at 6 to 12 months and a lower failure rate.
Hamstring Autograft ACL
Another excellent graft choice is the hamstring tendons located on the inside and just above the knee in the posterior aspect of the knee. In this surgery the gracillis and semitendinosus, which are two of the most easily available hamstrings, are harvested through a small incision just below the knee. These two tendons are then quadrupled and fixed in bone tunnels with a variety of different fixation devices. The hamstring autografts have an advantage of decreased donor site pain and problems, preservation of the extensor mechanism of the knee, excellent graft strength and are the preferred choice in young patients who are still growing.
The disadvantage of the hamstring is that without bone plugs they have slightly less secure initial fixation and some studies have shown increased laxity especially in females and mild hamstring weakness. In many parts of the country these are the procedures of choice for all athletes. However, they seem to be ideal in patients whose sports require frequent kneeling such as wrestlers and middle-aged athletes who would like autograft tissue, but do not want to go through the pain and rehabilitation of a bone-patella tendon graft.
Allograft ACL and Risk Factors
Allografts or cadaver grafts are often chosen for those patients who are older and those who are concerned with the smallest scar. When choosing an allograft tissue for an ACL reconstruction, we definitely recommend using an accredited tissue bank (ATB). At JOI we are very particular as to the source of our allografts and we have an exclusive relationship with the Musculoskeletal Transplant Foundation. They have reported no associated infections with almost two million units transplanted. Although allograft surgery represents a smaller procedure to the patient, more recent reports have indicated that these grafts do not have the same strength. Between six months and a year as autograft tissue and have a somewhat higher failure rate in active individuals.
ACL reconstruction surgery is a widely performed procedure to repair a torn anterior cruciate ligament in the knee. While the surgery is generally safe and effective, patients should be aware of potential risks and complications.
Common risks associated with ACL reconstruction surgery include infection, bleeding, blood clots, and adverse reactions to anesthesia. In rare cases, nerve or blood vessel damage may occur during the surgery. There’s also a small risk of developing a condition called arthrofibrosis, which involves excessive scar tissue formation in the knee joint.
To minimize risks and complications, it’s crucial to carefully follow the pre-operative and post-operative instructions provided by your surgeon. This may include taking certain medications, attending physical therapy sessions, and avoiding activities that could strain the knee during the recovery period.
Today’s ACL patients are very savvy. They often do their own internet research, and many make graft decisions depending on how their teammates or friends did with a particular type of procedure. There is no right or wrong answer to graft selection. However, in my practice BTB autografts are generally the choice for younger and more active patients. Hamstring grafts can also work for these same patients. Allograft tissue is usually chosen by older patients and females with cosmetic concerns. To read more about the ACL, please go to recovery from an ACL Surgery.
Recovery After ACL Reconstruction
Recovering from ACL reconstruction surgery requires a comprehensive approach that includes post-surgery rehabilitation and physical therapy, effective management of pain and discomfort, and an understanding of the timeline for recovery.
Post-surgery rehabilitation and physical therapy are key in restoring strength, flexibility, and stability to the knee. Your orthopedic surgeon or physical therapist will guide you through a personalized rehabilitation program tailored to your specific needs and goals. This program usually involves a combination of exercises, stretching, and functional training to gradually regain full range of motion and build up the muscles around the knee. Adhering to this program diligently is essential for a successful recovery. Physical therapy usually starts from 3 to 5 days after the procedure.
Managing pain and discomfort during the recovery process is vital for your overall well-being. Your healthcare provider may prescribe pain medications or recommend over-the-counter pain relievers to alleviate any post-surgery discomfort. Additionally, applying ice packs to the surgical site and elevating the leg can help reduce swelling and manage pain. It is important to follow your healthcare provider’s instructions regarding pain management to ensure a smooth recovery.
ACL Rehab Timeline.
The timeline for ACL reconstruction recovery varies for each individual, but generally, it takes several months to regain full function and return to sports or other physical activities. Initially, you may need to use crutches or a brace for support and limit weight-bearing activities. As your knee heals and strengthens, you will gradually progress to weight-bearing exercises and eventually resume normal activities. It is crucial to follow your healthcare provider’s guidance and not rush the recovery process to avoid re-injury or complications.
A physical therapy program will focus on early range of motion and quad strengthening. Rehab often allows patients to run at four months. Return to sports when quadriceps strength is 85-90% that of the uninjured leg. The average time to full recovery and return to sport, is between six months and a year. This depends on the athlete’s progress. Often there are some issues during the first year of participation following this surgery. High performance athletes may not return to their pre-injury status. However, most recreational athletes can return to their sport at some level. Associated injuries such as cartilage damage or meniscus tears often affect the clinical results. These may result in arthritis in years to come. The good news for most, is that the chances to return to play are greater now than ever before.

Returning to Activities after ACL Reconstruction
Returning to physical activities after ACL reconstruction surgery is a key milestone in the recovery process. However, it’s crucial to follow certain guidelines to ensure a safe and successful return to your favorite activities.
Firstly, consult with your orthopedic surgeon or physical therapist before resuming any physical activities. They will assess your progress and provide specific recommendations based on your individual case. Generally, you can expect to start with gentle exercises and gradually increase the intensity and duration over time.
When returning to sports, consider the specific requirements and potential risks associated with each activity. Sports like soccer, basketball, and football involve quick direction changes, pivoting, and jumping, which can put stress on the reconstructed ACL. It’s important to work closely with your physical therapist to develop a customized rehabilitation program that focuses on strengthening the surrounding muscles and improving stability.
The long-term outlook for ACL reconstruction patients is generally positive. With proper rehabilitation and adherence to the recommended guidelines, many individuals are able to return to their pre-injury level of activity and even participate in high-impact sports. However, each person’s recovery may vary, and it may take several months to a year to fully regain strength and confidence in the knee.

Common Questions About ACL Reconstruction
ACL reconstruction is a frequently performed surgical procedure used to repair a torn anterior cruciate ligament (ACL) in the knee. Here are some common questions about ACL reconstruction:
Who is a good candidate for ACL reconstruction?
A good candidate for ACL reconstruction is someone who has experienced a complete or partial tear of the ACL. This injury often occurs during sports activities that involve sudden stops, changes in direction, or direct impact to the knee. An orthopedic surgeon will assess the severity of the injury and determine if ACL reconstruction is the best course of action.
What are other treatment options for ACL injuries?
While ACL reconstruction is a common treatment for ACL injuries, there are other options depending on the severity of the injury and the patient’s goals. Non-surgical treatments, such as physical therapy, may be recommended for individuals with partial tears or less active lifestyles. However, ACL reconstruction is often the most effective method for restoring stability and function to the knee.
Do you have any success stories from ACL reconstruction patients?
At JOI Online, we have helped many patients get back to their active lifestyles through successful ACL reconstruction surgeries. Our patients have seen significant improvements in knee stability, range of motion, and overall quality of life. You can read some of our success stories and testimonials on our website to learn more about the positive outcomes of ACL reconstruction.
At JOI Online, we provide comprehensive resources and support for individuals undergoing ACL reconstruction. Our team of experts is dedicated to helping you navigate the recovery process and achieve optimal outcomes. Contact us today to learn more about our services and how we can assist you in your journey towards returning to your desired activities.
Learn more about ACL Reconstruction, go to this video.
- To schedule an appointment for physical or occupational therapy, call 904-858-7045 or 13 area JOI Rehab Centers.
JOI and JOI Rehab
JOI Physicians continue to offer online new patient appointments. Our physicians are Northeast Florida’s most respected orthopedic practice. To make an appointment by calling (904) JOI-2000 or schedule online. This is a new option to make it more convenient to make new patient appointments. Follow the link below to select your JOI MD and schedule online.

By: Tim Wall, MS, ATC